
ST. LOUIS MEDIA
Riverfront Times coverage
Riverfront Times published a St. Louis article on CockfightUSA and Missouri intactivist outreach in July 2023.
This is not a random one-day protest. Missouri-area intactivist outreach has already drawn local radio, television, and St. Louis media attention. These examples help reporters see the regional context before covering the July 2026 Bloodstained Men tour.
Riverfront Times published a St. Louis article on CockfightUSA and Missouri intactivist outreach in July 2023.

Kansas City-area radio coverage shows that the issue can work as a live discussion topic, especially when framed with a local spokesperson and a clear public-interest angle.

Prior Missouri-area actions produced clear visual material for local TV. Bloodstained Men protests also provide strong street visuals, signage, and interview opportunities.
Protesters oppose routine, non-therapeutic circumcision of infants and minors when there is no immediate medical necessity and the child cannot personally consent.
The protest is not about medically necessary treatment for a diagnosed condition. It focuses on routine infant circumcision performed for cultural, social, religious, or claimed preventive reasons.
Activists argue that irreversible surgery on healthy genital tissue should be delayed unless medically necessary, so the person affected can decide for himself when older.
The campaign asks journalists to separate emergency medical need from preventive claims, cultural assumptions, billing incentives, and informed-consent gaps.
This story touches medicine, parenting, religion, law, bodily autonomy, protest speech, public health messaging, and children’s rights. That is exactly why it needs careful reporting instead of assumptions.
This section gives a newsroom-friendly overview: what is happening, why it is visual, who can speak, and where to verify details before sending a crew.
William Erker is available to explain the protest, the local outreach effort, and why activists are asking media to examine routine infant circumcision as a consent and medical-ethics issue.
Replace this line with William’s public media contact:
Phone: [William media phone]
Email: [William media email]
Reporters can use this page to access background context, citations, prior Missouri coverage, tour details, visuals, and interview scheduling.
Main media URL:
https://nextlevelintactivism.com/media/
This section is ready for new material once the Mid South tour begins. Add protest photos, short video clips, published articles, broadcast segments, and interview clips here.
Coming soon: St. Louis protest images and field photos.
Coming soon: short clips for editors, producers, and social media reference.
Coming soon: links to articles, radio segments, TV clips, and interviews.
The official Bloodstained Men schedule should be treated as the source of truth. Exact locations may change on short notice, so reporters should verify before sending a crew.
| Date | City | Time | Location | Media Note |
|---|---|---|---|---|
| Wed, July 22, 2026 | St. Louis, MO | 10am–12pm | TBA | Primary St. Louis media target |
| Wed, July 22, 2026 | Fairview Heights, IL | 2pm–4pm | Lincoln Hwy & N Illinois St | Metro East / St. Louis regional angle |
| Mon, July 27, 2026 | Joplin, MO | 1pm–2:30pm | S Rangeline Rd & E 7th St | Southwest Missouri outreach |
| Mon, July 27, 2026 | Springfield, MO | 4pm–5:30pm | E Battlefield Rd & S Glenstone Ave | Springfield media outreach |
| Tue, July 28, 2026 | Kansas City, MO | 10am–TBA | TBA | Prior KC coverage hook |
| Tue, July 28, 2026 | Sedalia, MO | TBA | W Broadway Blvd & S Limit Ave | Central Missouri stop |
| Wed, July 29, 2026 | Columbia, MO | 9:30am–11am | E Nifong Blvd & S Providence Rd | College-town / public debate angle |
| Wed, July 29, 2026 | Jefferson City, MO | 12:30pm–2pm | Missouri Blvd & Hwy 50 | State capital / policy angle |
| Wed, July 29, 2026 | Wentzville, MO | 4pm–5:30pm | W Pierce Blvd & Wentzville Pkwy | Greater St. Louis regional follow-up |
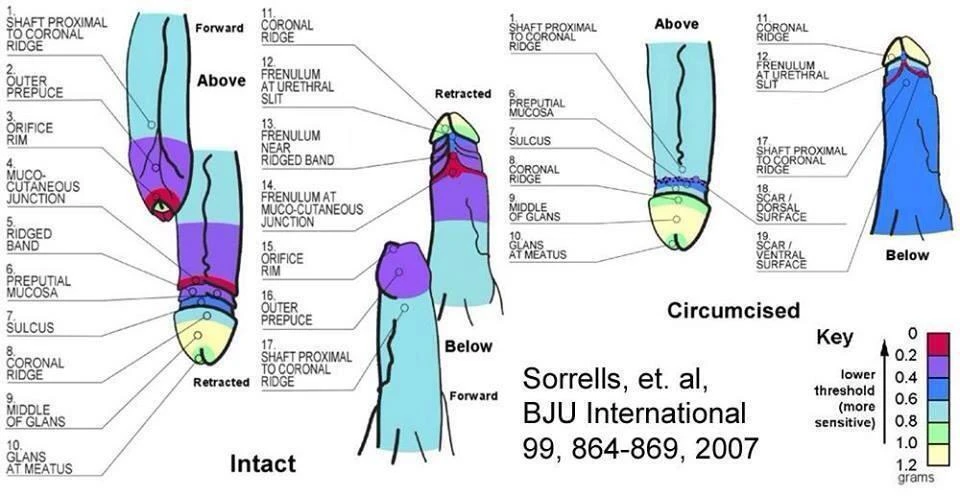
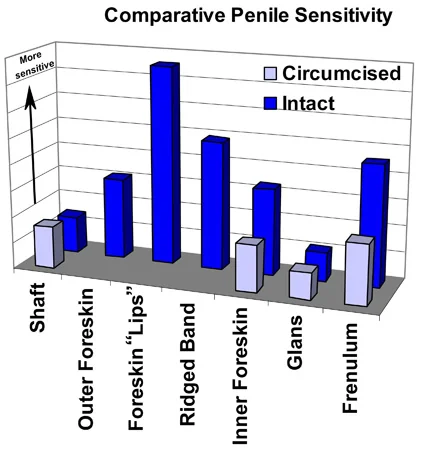
Sensory mapping, histology, mechanical function, and tissue-loss scale. Expand sections to view key visuals and primary sources.
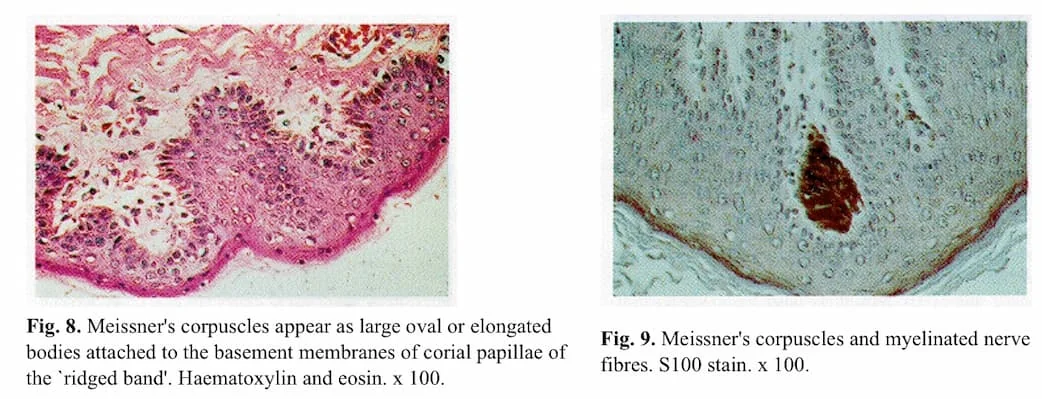
Key point: Fine-touch sensitivity is not uniform. It clusters in specific anatomical regions. The sensitivity mapping in Sorrells et al. (2007) is consistent with what histology papers describe about preputial tissue: specialized mucosa and sensory structures, including mechanoreceptors, concentrated in specific regions.
A mechanical analysis of intromission explains how an unretracted foreskin functions as a folded, low-friction interface. As the penis advances, the foreskin “unrolls” so initial contact occurs on tissue already positioned along the shaft before direct friction occurs between the device or introitus and the skin. In the study’s experimental setup, repeated measurements reported a 10-fold reduction in entry force with an initially unretracted foreskin compared with a retracted foreskin.


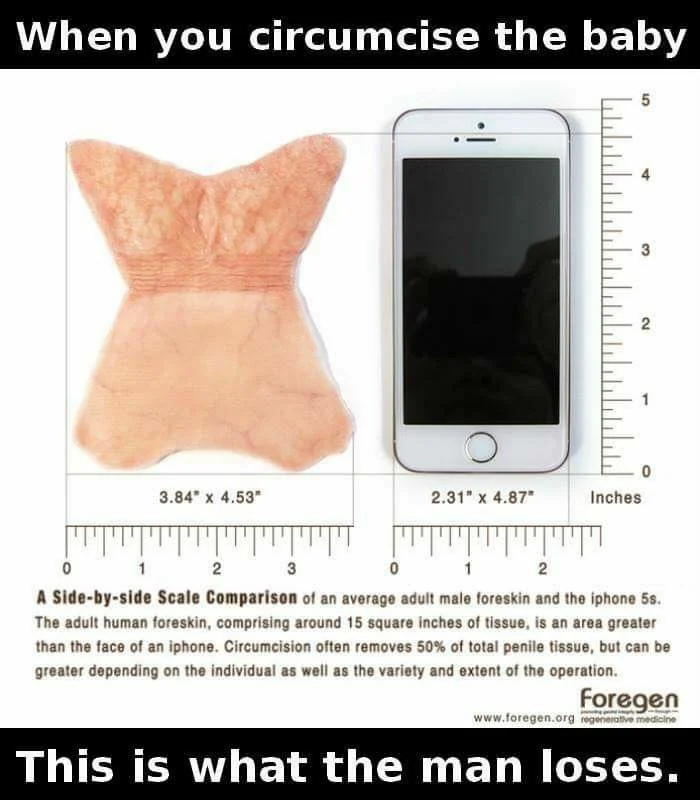
Many people are told this is a “small snip.” In reality, this is commonly described as removing roughly 1/3 to 1/2 of penile tissue surface area — often cited as roughly 12–18 square inches in adult equivalents. In the intact adult male, this tissue everts during erection, becoming the primary interfacing tissue that both gives and receives sensation during intercourse.
Infant pain, stress physiology, trauma research, and long-term neurodevelopmental questions. Expand sections to review evidence, references, and warning-gated images of infant distress indicators.
Infants experience pain and process noxious stimuli in the brain. Modern research shows patterns of brain activity consistent with pain processing, and newborns can exhibit strong physiological stress responses during painful procedures.
Facial tension, vocal intensity, muscle rigidity, and behavioral shutdown are widely recognized distress indicators in infants. The claim “they won’t remember” confuses conscious recall with biological and neurological impact.
Research measuring cortisol before and after circumcision reports a significant neonatal stress response. In the cited cortisol study, dorsal penile nerve block did not eliminate the cortisol elevation associated with the procedure, indicating stress signaling persisted despite regional anesthesia.
A widely cited study reported that circumcised infants showed higher pain scores and longer crying during routine vaccination at 4–6 months, suggesting early severe pain may amplify later pain response.
A 1982 observational study reported differences in feeding patterns following circumcision and suggested that some infants appeared less available for social interaction afterward. Note: that study used bottle-feeding, and breastfeeding is more physically demanding than bottle-feeding.
Severe or repeated stress in early life can influence neurodevelopment, stress regulation, and later health vulnerability. These effects do not require explicit memory to become biologically embedded.
Newer early-life adversity research supports the broader developmental logic: early stress exposure can be associated with changes in brain development, structure-function coupling, stress regulation, and behavioral outcomes. This research does not need to be circumcision-specific to be relevant to the biological question: whether early pain and stress can matter even when a child has no later conscious memory.
A pediatric neuroimaging study modeled structural-functional brain connectivity across childhood and reported adversity-linked differences consistent with altered neurodevelopmental timing.
A Molecular Psychiatry review summarizes evidence that adversity can shape brain structure and function, with implications for development, adaptation, and later mental-health vulnerability.
Harvard’s Center on the Developing Child describes toxic stress as prolonged activation of stress-response systems that can disrupt healthy brain architecture and other biological systems.







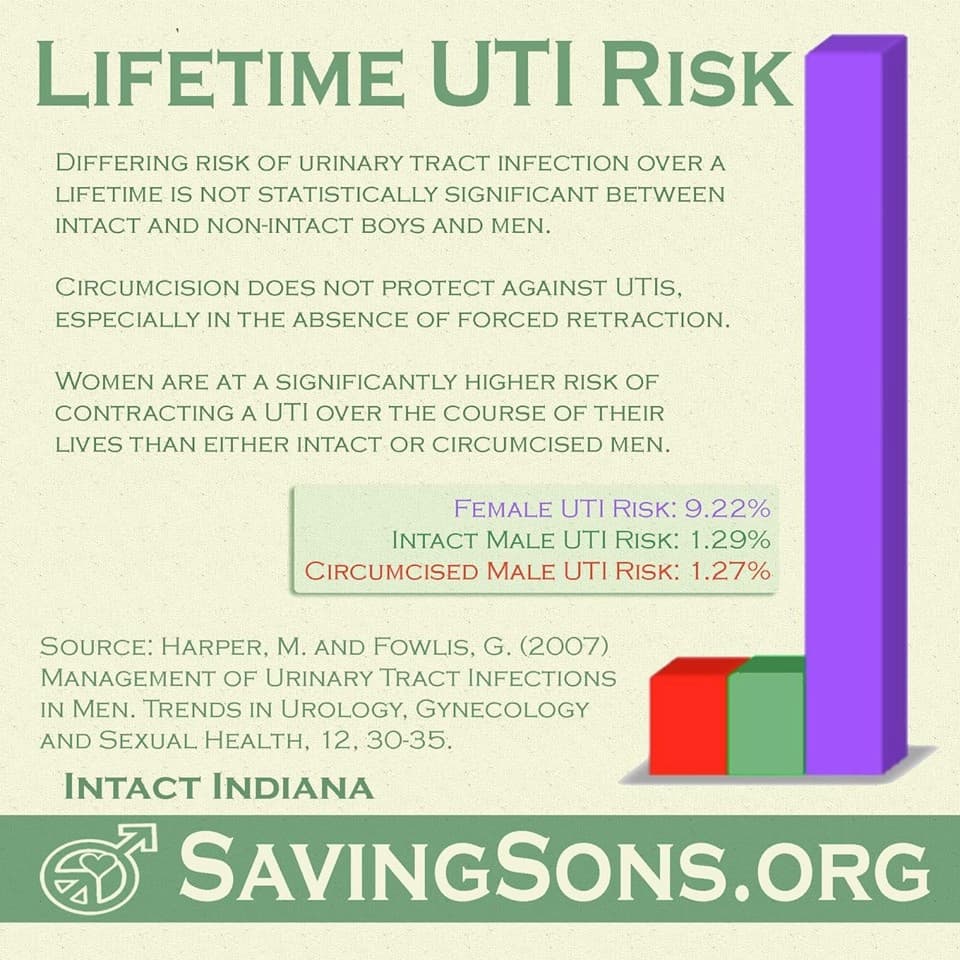
A reality check on UTI, “phimosis,” STI/HPV, HIV, and cancer claims — with the confounders journalists should interrogate: forced retraction injuries, diagnostic bias, absolute risk, consent-based alternatives, and population-level outcomes.
Veterinary anatomy describes the prepuce as the normal sheath of the flaccid penis in mammals. If routine “preventive” prepuce amputation were medically necessary, you would expect it to appear as standard veterinary practice. It does not. That is a giant red flag for the “default = disease” framing.

Translation for reporters: if a study never controlled for forced retraction practices, it may be measuring clinician-caused harm, not “foreskin risk.”
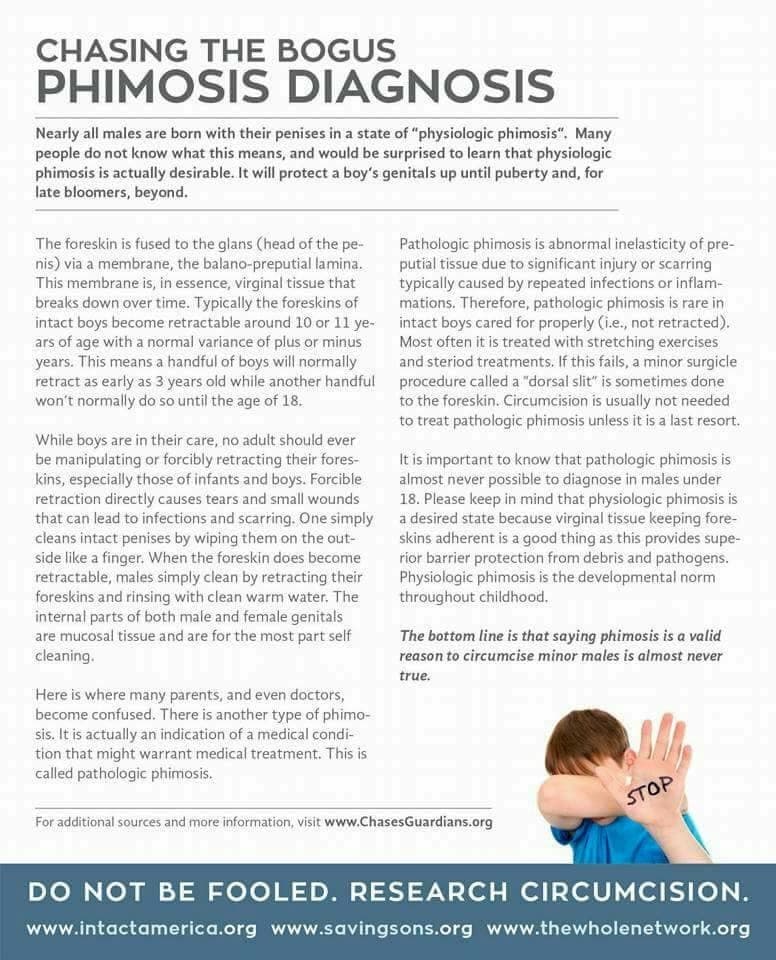
The “phimosis” narrative is often where bad anatomy education turns into bad medicine. If clinicians push retraction too early, tears and scarring follow — then “phimosis” appears later as a self-fulfilling outcome.
If someone is trying to sell circumcision as “HPV prevention,” ask why they are skipping the intervention that directly targets HPV: vaccination. CDC states that HPV vaccination can prevent over 90% of cancers caused by HPV.
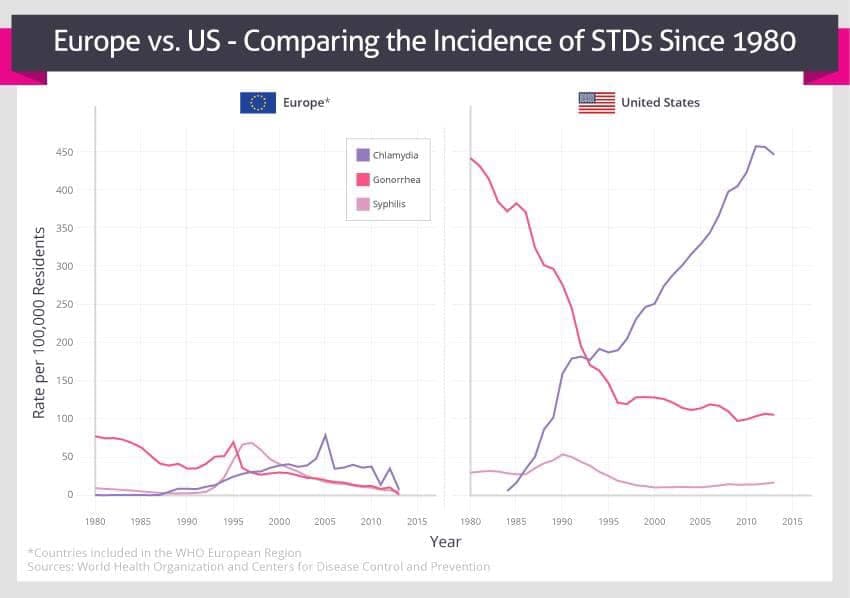
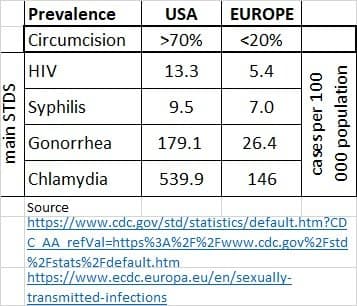
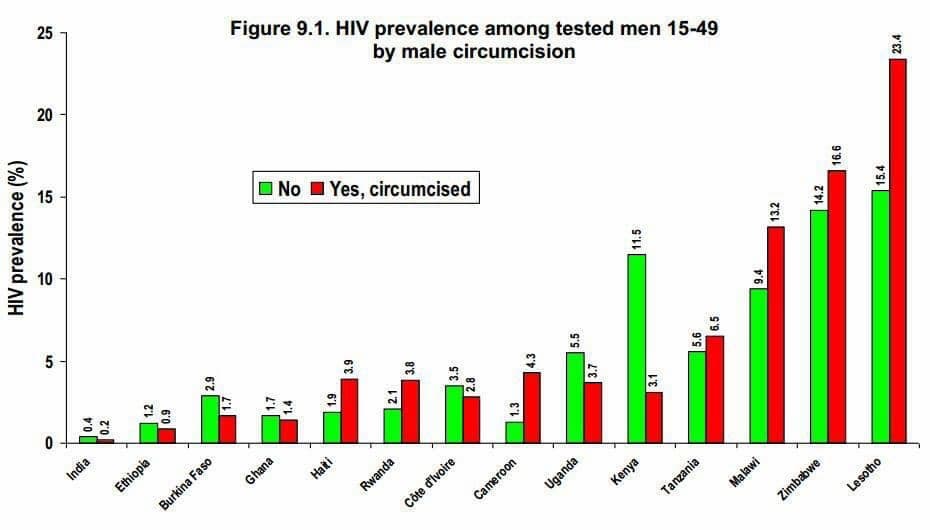
Population reality check: if circumcision were a dominant driver of better sexual-health outcomes, low-circumcision countries would show obvious worsening trends. That pattern is not consistently observed.
Mechanically, removing a mobile tissue sheath changes how intercourse works: gliding motion, moisture environment, and friction. If this were framed purely as a sexual-health device problem instead of a cultural ritual, it would never be pitched as routine medicine.
If someone cites adult trials in specific high-prevalence settings, ask whether those findings are being generalized to newborns and to completely different epidemiological contexts. That leap is the story.
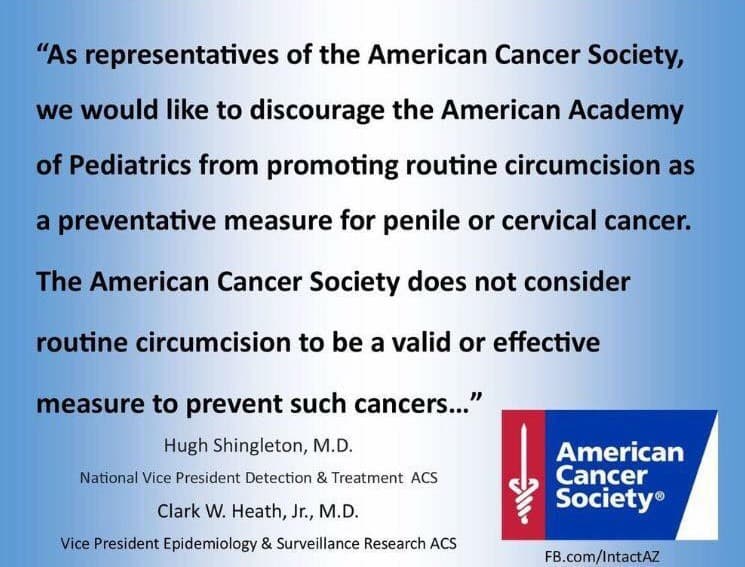
Penile cancer is uncommon in developed countries. Reporters should demand incidence rates and the number-needed-to-treat, then compare that to the harms and to modern prevention such as HPV vaccination, hygiene, and treatment of inflammation.
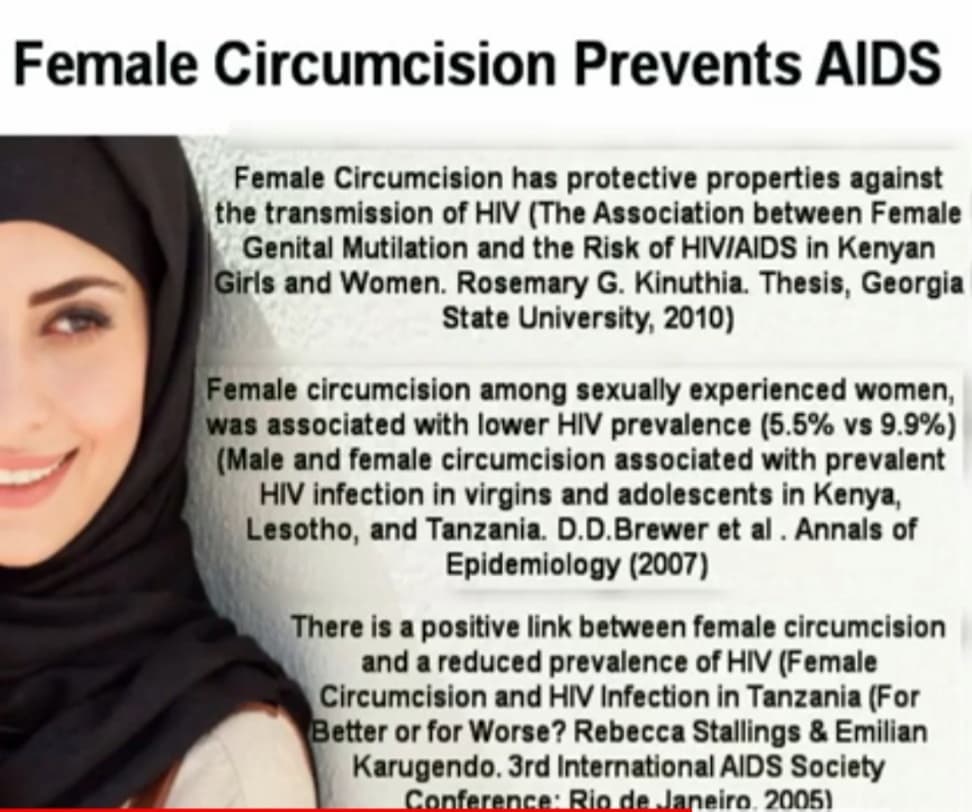
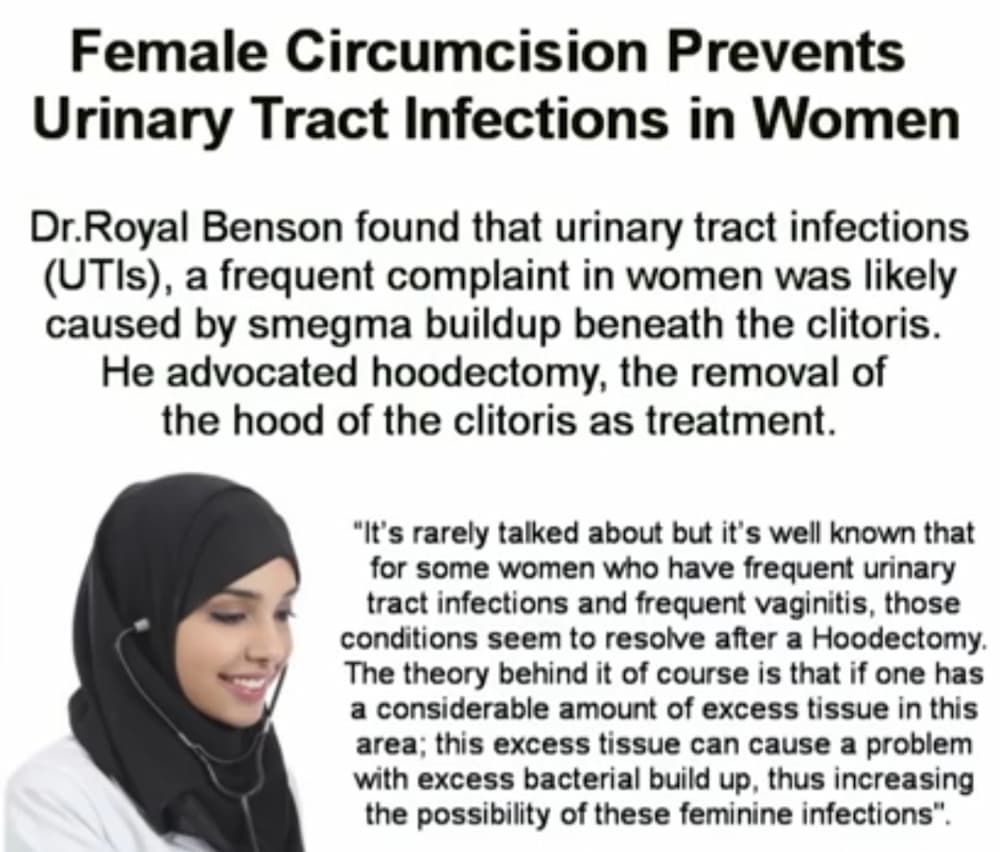
Newsroom-facing background on how harmful practices persist through normalization, taboo enforcement, medical rebranding, legal collisions, knowledge suppression, and consent double standards — with concrete examples reporters can investigate.
Establish the “normal here / unthinkable elsewhere” dynamic: painful practices can persist when recoded as love, duty, beauty, grief management, or identity — independent of biomedical justification.
Journalist question: When does cultural respect enable preventable harm?

Explain persistence mechanisms without pathologizing individuals or asserting motive certainty. The focus is on repeatable dynamics: dissonance management, identity protection, and social proof.
Journalist question: What social cost is attached to admitting harm — and who pays it?
Show how medical language can function as cultural “armor”: shifting the frame from bodily harm to consumer service and purported health protection.
Journalist question: Would this claim survive evidence review if it were any other body part?

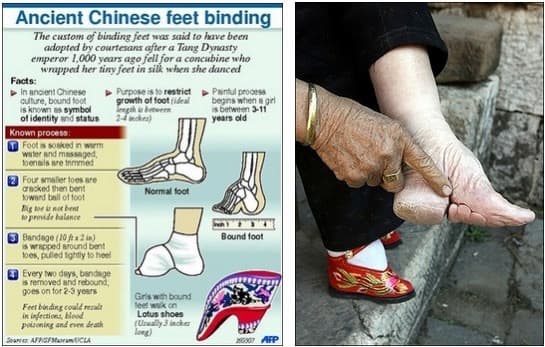
Show recurring persistence logic across cultures and time: a practice can be framed as virtue or beauty, reinforced by status incentives, and maintained by stigma — until incentives change.
Journalist question: Which ending mechanism applies here?

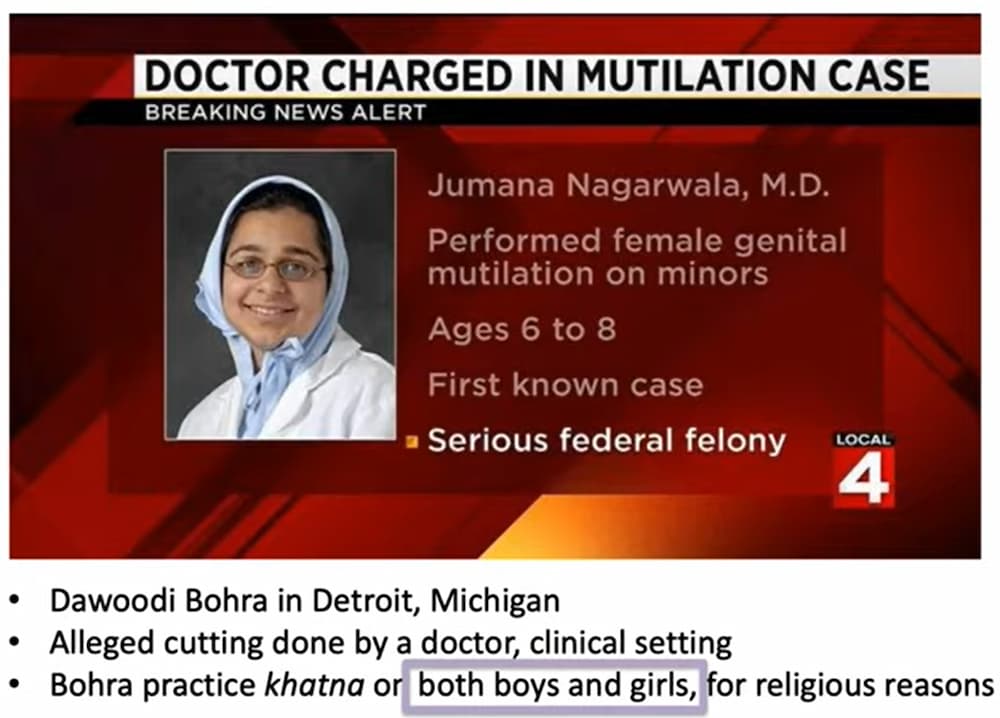
Make the legal collision the turning point. The goal is accuracy: distinguish what the federal dismissal decided — constitutional authority / jurisdictional design — from broader ethical or policy questions that remain disputed.
Journalist question: When cultural exemption creates legal inconsistency, what gets protected in practice?
Connect social taboos to medical education failures: what is not discussed tends not to be taught. When “normal anatomy” becomes optional knowledge, errors can become routine — and routine becomes invisible.
Journalist question: What do training materials say today — and what do clinics do tomorrow morning?
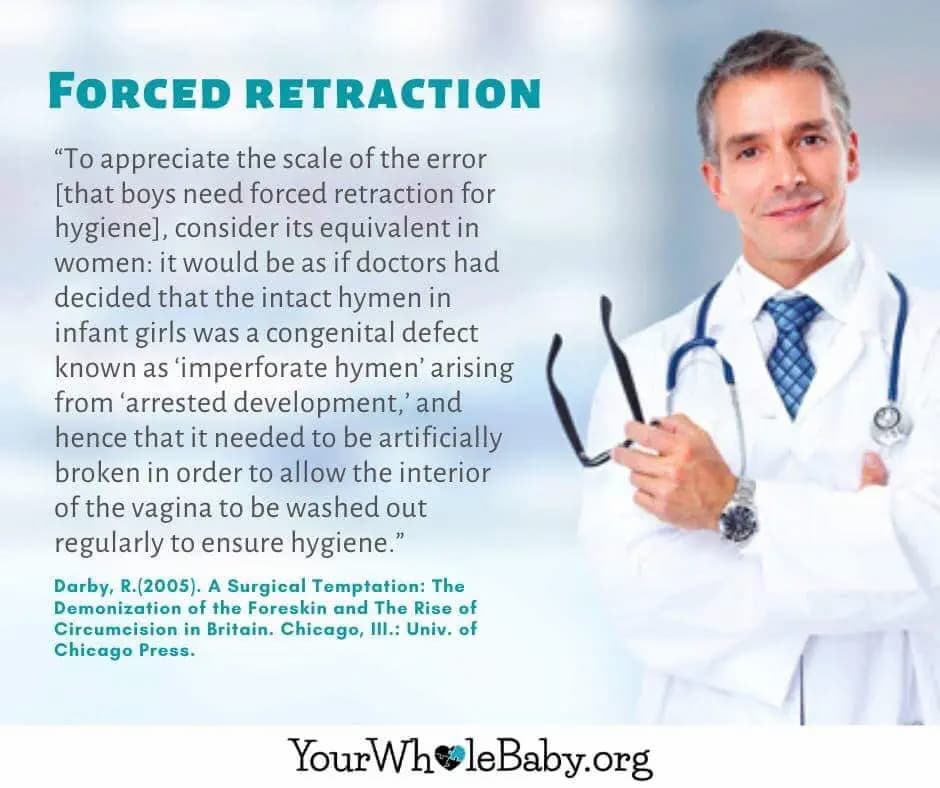
Provide a concrete example of preventable harm. Forced retraction is a standard-of-care issue with institutional guidance emphasizing that infant foreskin should not be forcibly retracted.
Journalist question: Is iatrogenic harm being miscounted as “anatomy pathology”?
Close the systemic loop: routine/high-volume procedures can become “default solutions” even when education on anatomy, function, and non-invasive alternatives is incomplete.
Journalist question: What competencies are required — and how are they assessed?

Provide newsroom-safe ethical framing: a classification distinction between therapeutic treatment for diagnosed pathology and prophylactic, irreversible intervention on a non-consenting patient. This framing focuses on consent and consistency rather than directives.
Final newsroom question: What standard do we want to normalize — and who is unable to consent to it?
